
It’s 2 AM. You’re rocking the baby, exhausted beyond belief, but your heart is hammering against your ribs like a trapped bird. You’re sweating through another shirt despite the cool night air, and your hands won’t stop shaking. You tell yourself it’s just the stress of new motherhood. Maybe it’s caffeine. But deep down, something feels off. This isn’t just tiredness; it’s physical.
If this sounds familiar, you might not be dealing with standard postpartum adjustment or even postpartum depression, which affects mood primarily. You could have postpartum thyroiditis, an autoimmune condition that disrupts your thyroid gland within the first year after childbirth. It affects roughly 5 to 10 percent of women, yet many go undiagnosed for months because their symptoms are mistaken for normal mom fatigue or mental health struggles.
Key Takeaways
- Biphasic Pattern: Most cases start with hyperthyroidism (overactive) followed by hypothyroidism (underactive), though some experience only one phase.
- Silent Mimic: Symptoms often overlap with postpartum depression, leading to misdiagnosis in up to 30% of cases.
- Diagnosis is Simple: A blood test checking TSH, Free T4, and TPO antibodies can confirm the condition early.
- Recovery is Likely: About 70-80% of women return to normal thyroid function within 12-18 months without permanent damage.
- Risk Factors Matter: Having Type 1 diabetes or existing thyroid antibodies significantly increases your risk.
What Is Postpartum Thyroiditis?
Postpartum thyroiditis is an inflammatory disease of the thyroid gland triggered by immune system changes after pregnancy. During pregnancy, your immune system suppresses itself slightly to protect the baby. After delivery, it rebounds aggressively. In some women, this rebound goes haywire, causing anti-thyroid antibodies-specifically TPO antibodies (thyroid peroxidase antibodies)-to attack the thyroid tissue.
This attack damages the thyroid follicles, causing stored hormones to leak into the bloodstream. This initial surge creates a temporary state of hyperthyroidism. Once those stores are depleted, the damaged gland can’t produce enough hormone, leading to hypothyroidism. Unlike Graves’ disease, which also causes hyperthyroidism, postpartum thyroiditis is painless and does not cause eye problems (ophthalmopathy).
Historically described in the 1940s, this condition gained clinical clarity in the 1960s and 70s with better antibody testing. Today, we understand it as a distinct entity from chronic Hashimoto’s thyroiditis, although they look identical under a microscope. The key difference? Postpartum thyroiditis is often temporary.
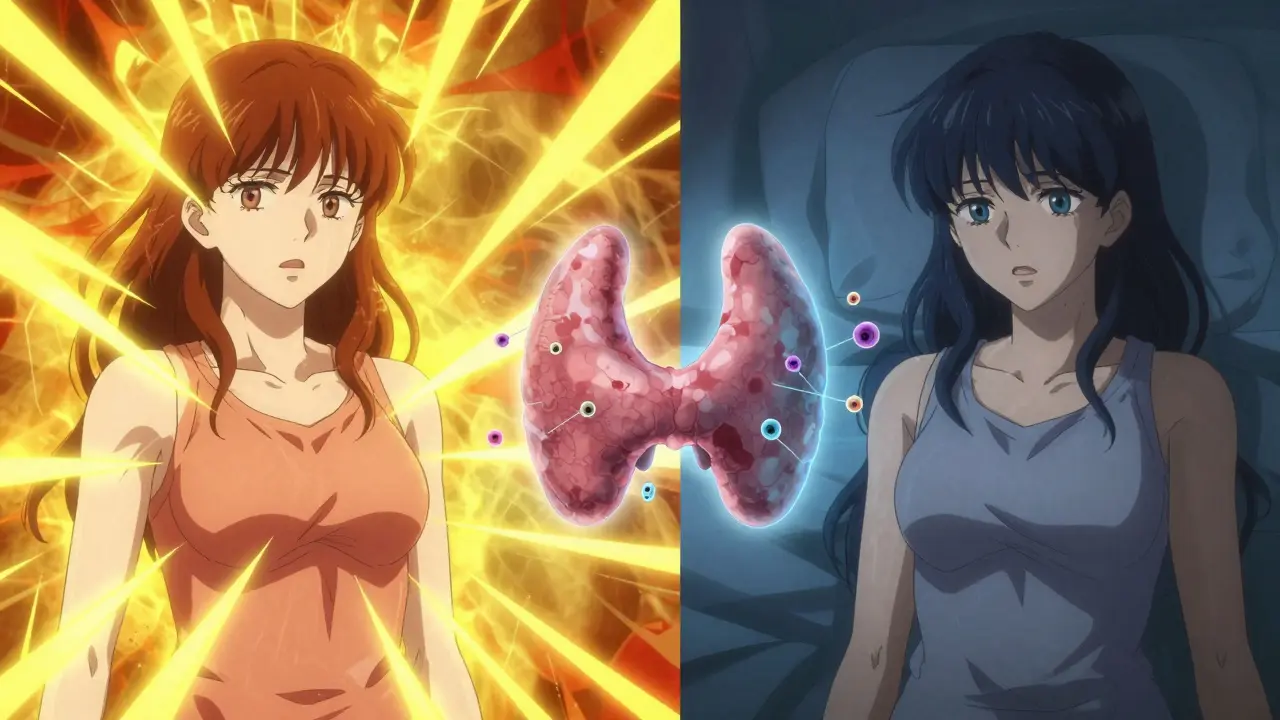
The Two Phases: What to Expect
Understanding the timeline is crucial because the symptoms flip-flop. If you know what’s coming, you can advocate for yourself better. Here is how the biphasic pattern typically unfolds:
Phase 1: Hyperthyroidism (Weeks 1-4)
This phase usually begins between 1 and 4 months postpartum. Your body is flooded with excess thyroid hormone due to leakage from the inflamed gland. You might feel wired, anxious, or irritable. Physical signs include:
- Heat intolerance: Feeling hot when others are comfortable.
- Tachycardia: Heart rate exceeding 100 beats per minute at rest.
- Weight loss: Dropping 4-7 pounds unintentionally.
- Tremors: Shaky hands, especially when holding objects.
- Insomnia: Difficulty sleeping even when the baby sleeps.
Note that up to 50% of women have mild or no symptoms in this phase, so it’s often missed entirely.
Phase 2: Hypothyroidism (Months 4-8)
As the hormone stores run dry, the pendulum swings the other way. This phase peaks around 6 months postpartum and can last for several months. Now, your metabolism slows down drastically. Symptoms include:
- Profound fatigue: Exhaustion that doesn’t improve with sleep.
- Cold intolerance: Feeling chilly in warm rooms.
- Brain fog: Trouble concentrating or remembering simple tasks.
- Hair loss: Thinning hair on the scalp.
- Constipation and dry skin.
- Weight gain: Gaining 5-10 pounds despite diet changes.
About 10-25% of women skip the hyperthyroid phase and go straight to hypothyroidism. Another small group experiences only the initial hyperthyroid spike and recovers quickly.
Postpartum Thyroiditis vs. Postpartum Depression
This is the most critical distinction to make. Both conditions share symptoms like fatigue, irritability, and difficulty concentrating. However, they require completely different treatments. Misdiagnosis is common; studies suggest nearly 30% of women with postpartum thyroiditis are initially treated for depression alone.
| Feature | Postpartum Thyroiditis | Postpartum Depression |
|---|---|---|
| Primary Cause | Autoimmune inflammation of thyroid | Neurochemical/hormonal shifts affecting mood |
| Physical Symptoms | Prominent: Heart palpitations, temperature sensitivity, weight changes | Less prominent: Sleep/appetite changes may occur but less specific |
| Mood Symptoms | Anxiety (hyper phase), sadness/apathy (hypo phase) | Persistent sadness, hopelessness, guilt, anxiety |
| Diagnostic Test | Blood test: TSH, Free T4, TPO Antibodies | Clinical interview and screening questionnaires (e.g., Edinburgh Scale) |
| Treatment | Observation, beta-blockers (rarely), or levothyroxine | Therapy, antidepressants, support groups |
If you have been diagnosed with postpartum depression but still feel physically unwell-with racing heart, cold intolerance, or unexplained weight changes-ask your doctor for a thyroid panel. Treating the thyroid issue may resolve both the physical and emotional symptoms.
Who Is at Risk?
Not every woman develops this condition. Certain factors significantly increase your likelihood of developing postpartum thyroiditis:
- Type 1 Diabetes: Women with Type 1 diabetes have a 25-30% chance of developing this condition due to shared autoimmune pathways.
- Positive TPO Antibodies: If you tested positive for thyroid peroxidase antibodies before or during pregnancy, your risk jumps to about 70%.
- History of Thyroid Disease: Previous thyroid issues or a prior episode of postpartum thyroiditis increase recurrence rates to 40%.
- Family History: Autoimmune diseases running in your family raise your susceptibility.
Experts like Dr. Rebecca Smith from UR Medicine note that testing for TPO antibodies at 10 weeks postpartum in high-risk women can predict 70% of subsequent cases. Early identification allows for proactive monitoring rather than reactive crisis management.
Diagnosis and Testing
Diagnosis relies on blood tests, not just symptoms. Because symptoms overlap so much with normal postpartum life, objective data is essential. The standard protocol involves:
- TSH (Thyroid Stimulating Hormone): Low TSH indicates hyperthyroidism; high TSH indicates hypothyroidism.
- Free T4 (Thyroxine): Elevated in the hyper phase, low in the hypo phase.
- TPO Antibodies: Positive results confirm the autoimmune nature of the disorder. About 80-90% of affected women test positive.
The American Thyroid Association recommends testing symptomatic women at 6-12 weeks postpartum. While routine universal screening is debated, many endocrinologists now advocate for baseline testing in high-risk groups. If you fall into the high-risk category, don’t wait for symptoms to become severe. Ask for these tests at your postpartum checkup.
Treatment and Management
The good news? There is no cure needed because the condition is self-limiting for most. Treatment focuses on managing symptoms while your thyroid heals.
During the Hyperthyroid Phase
Antithyroid medications (like methimazole) used for Graves’ disease are not effective here because the problem is hormone leakage, not overproduction. Instead, doctors may prescribe:
- Beta-blockers: To control rapid heartbeat and tremors if symptoms are severe.
- Rest and Hydration: Supporting your body through the metabolic surge.
During the Hypothyroid Phase
If your TSH rises significantly (usually above 10 mIU/L) or you have severe symptoms, your doctor may prescribe levothyroxine, a synthetic thyroid hormone. This helps alleviate fatigue, brain fog, and depression-like symptoms. Importantly, levothyroxine is safe for breastfeeding.
Once your thyroid function returns to normal, you will likely taper off the medication. However, 20-30% of women develop permanent hypothyroidism and will need lifelong therapy. Regular follow-up blood tests every 4-6 months for the first year are crucial to adjust dosage or discontinue treatment safely.
Living With Postpartum Thyroiditis
Navigating this condition while caring for a newborn is emotionally taxing. Many women report feeling gaslit by healthcare providers who dismiss their complaints as "just being a new mom." You are not crazy. Your symptoms are real and physiological.
Practical tips for coping:
- Track Your Symptoms: Keep a log of heart rate, weight, temperature preferences, and mood. This data helps your doctor see patterns.
- Advocate for Blood Work: If you feel wrong, insist on testing. Don’t accept "it’s all in your head" as an answer.
- Support Your Metabolism: Eat nutrient-dense foods. Avoid excessive caffeine, which can worsen anxiety and heart palpitations during the hyper phase.
- Connect With Others: Online communities, such as those on Reddit or HealthUnlocked, provide validation and practical advice from women who have walked this path.
Remember, recovery is highly probable. For the vast majority, thyroid function normalizes within 12 to 18 months. Even if you end up with permanent hypothyroidism, it is easily managed with daily medication, allowing you to live a fully healthy life.
Is postpartum thyroiditis dangerous?
For most women, it is not life-threatening, but untreated severe hyperthyroidism can strain the heart, and severe hypothyroidism can lead to myxedema coma (rare). More commonly, the danger lies in misdiagnosis, where physical symptoms are ignored, worsening quality of life and bonding with the baby.
Can I breastfeed with postpartum thyroiditis?
Yes, breastfeeding is generally safe. However, during the hypothyroid phase, low thyroid levels can sometimes decrease milk supply. Taking prescribed levothyroxine is safe for breastfeeding and may help restore energy and supply.
Will I get postpartum thyroiditis again in future pregnancies?
If you have had it once, your risk of recurrence in subsequent pregnancies is approximately 40%. If you have positive TPO antibodies, the risk is even higher. Monitoring thyroid function closely in future pregnancies is recommended.
How long does postpartum thyroiditis last?
The entire process typically lasts 12 to 18 months. The hyperthyroid phase lasts 1-3 months, followed by the hypothyroid phase lasting 6-12 months. About 70-80% of women recover full thyroid function; 20-30% remain hypothyroid permanently.
Should I take iodine supplements?
No. Excess iodine can worsen autoimmune thyroid conditions. Stick to a balanced diet unless your doctor specifically prescribes otherwise. Focus on selenium and zinc, which support thyroid health, but consult your provider before adding any supplements.






rebecca torres
June 14, 2026 AT 03:17look i had this shit after my second kid and nobody believed me for six months. they kept telling me it was just postpartum depression or that i needed to sleep more. classic gaslighting. i finally forced my gp to run the tpo antibodies test because my heart was literally racing at rest while i was trying to fold laundry. turns out my tsh was like 0.1 and free t4 through the roof. once we got that confirmed, everything made sense. dont let them dismiss you as crazy mom. demand the blood work.
Emily Barnhill
June 15, 2026 AT 23:11Rebecca is absolutely right about the dismissal from healthcare providers, but I want to add a layer of nuance here for anyone reading this who feels overwhelmed by the medical jargon. It is crucial to understand that your body is undergoing a massive immune rebound, not a character flaw. When Emily Barnhill talks about forcing the GP, she means advocating firmly, not necessarily being hostile, though sometimes firmness is required when empathy fails in clinical settings.
I’ve seen too many women internalize the fatigue as failure. Please remember that the biphasic nature of this condition means your symptoms will shift. If you are currently feeling wired and anxious, that is likely the hyperthyroid phase leaking hormones. If you are crashing into deep exhaustion and brain fog, you may be entering the hypothyroid phase. Tracking these shifts in a simple journal can provide objective data that doctors cannot argue with. You are not imagining this. Your physiology is screaming for attention, and listening to it is an act of self-preservation, not selfishness. Let’s create a space where we validate each other’s physical reality without judgment.
Hailey Dunston
June 17, 2026 AT 12:26Oh, how quaint. The notion that one must 'advocate' so aggressively for basic care suggests a systemic failure that most educated individuals simply navigate around. One does not need to 'force' a physician; one merely needs to present the correct diagnostic criteria with sufficient intellectual weight.
The article mentions TPO antibodies, which is elementary immunology, yet laypeople treat it as groundbreaking news. It is rather tedious to watch people reinvent the wheel every decade. If you have Type 1 diabetes, as noted, your risk is nearly 30%. This is not a mystery; it is statistical probability. Those who fail to monitor their thyroid function postpartum are essentially gambling with their endocrine health due to a lack of prior education. Perhaps if we elevated the discourse beyond emotional venting, fewer women would suffer from preventable misdiagnoses. But then again, simplicity often appeals more than precision. :)
Christina S.
June 18, 2026 AT 16:09Hey Hailey, I get that you’re frustrated, but coming across as elitist doesn’t help the women who are genuinely scared and confused. Most of us aren’t immunologists. We’re tired moms trying to figure out why we feel like zombies while everyone else says we should be happy.
Emily and Rebecca, thank you for sharing your experiences. It really helps to know I’m not alone in feeling dismissed. I’m currently in month 3 postpartum and my hands won’t stop shaking. I thought it was just caffeine withdrawal since I cut back on coffee, but now I’m wondering if it’s the hyper phase. Should I push for testing even if my OB says I look fine? I don’t want to be annoying, but I also don’t want to ignore something real.
Brett Webster
June 20, 2026 AT 00:47Christina, you are definitely not being annoying. In fact, you are being proactive, which is exactly what you should be doing. As someone who works in healthcare administration, I see this all the time. Visual appearance tells a doctor nothing about your internal hormone levels. You can look perfectly healthy and still have severe thyroid dysfunction.
If you are experiencing tremors, heat intolerance, or palpitations, those are textbook signs of the hyperthyroid phase. Do not wait for your next scheduled appointment if you can avoid it. Call your provider and specifically ask for a thyroid panel: TSH, Free T4, and TPO antibodies. Mention that you suspect postpartum thyroiditis based on your symptoms. Using specific terminology often prompts a different response from clinicians than saying 'I feel weird.' Trust your instincts. They are usually right.
Erin Livengood
June 21, 2026 AT 08:59There is a profound irony in how we treat new mothers. We celebrate the miracle of birth but pathologize the biological aftermath. The body undergoes a seismic shift, a violent recalibration of immunity and metabolism, and yet we expect silence and grace. Postpartum thyroiditis is not just a medical condition; it is a testament to the sheer physical cost of creation.
When we speak of 'brain fog,' we are speaking of the mind struggling to anchor itself in a sea of hormonal flux. It is not laziness. It is survival. I find comfort in knowing that this storm passes, that the pendulum swings back. But until it does, we must be our own fierce guardians. We must demand the tests, track the numbers, and refuse to be minimized. Our bodies are not machines to be fixed; they are landscapes to be navigated with respect and vigilance.
Aditya Singh
June 23, 2026 AT 00:14Excellent points Erin. From a clinical perspective in India, we often see delayed diagnoses because patients attribute symptoms to cultural norms of postpartum weakness or stress. However, the biochemical markers remain universal. The key takeaway here is the importance of serial monitoring. A single normal TSH at 6 weeks does not rule out PPT if symptoms persist. We recommend checking at 3, 6, and 12 months for high-risk cohorts. Early intervention with beta-blockers for symptomatic relief during the thyrotoxic phase can significantly improve quality of life. Remember, levothyroxine is safe for lactation, so do not hesitate to treat the hypothyroid phase if it arises. Your milk supply and mental well-being depend on adequate thyroid hormone levels.
Glenn Davis
June 24, 2026 AT 08:43Healthcare systems are failing basic duties. Simple blood tests ignored. Women suffering unnecessarily. Fix the system. Stop blaming patients for advocating. Doctors need to follow protocols. No excuses.
Cici arya Arya
June 26, 2026 AT 01:45I am so sorry you are going through this Christina. It sounds incredibly draining. I had similar issues and felt so isolated. My husband didn't understand why I was sweating in winter. He thought I was overreacting. It took forever to get diagnosed. I hope you get the answers you need soon. Please take care of yourself and don't let anyone tell you it's all in your head. You deserve better care. Sending you strength and hugs. ❤️